Management

A guideline-based approach to allergic rhinitis (AR) treatment
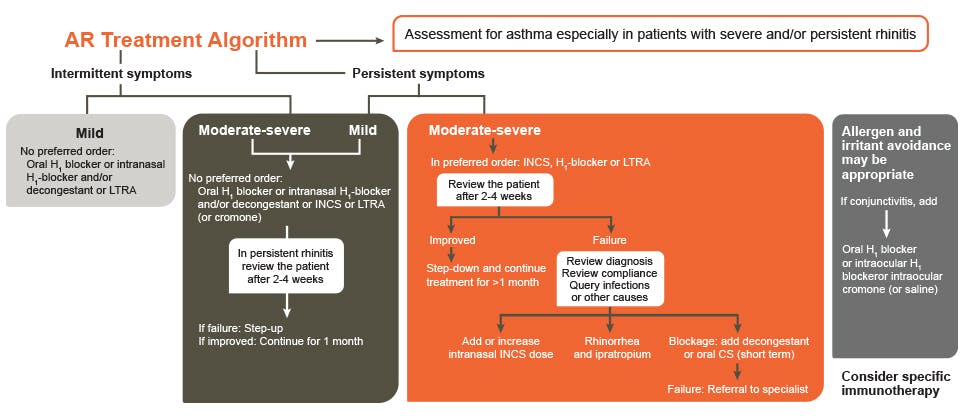
ARIA AR treatment algorithm1
The management of AR should be tailored according to the severity of the disease, co-morbidities, treatment availability and affordability, and the patient’s preference.1
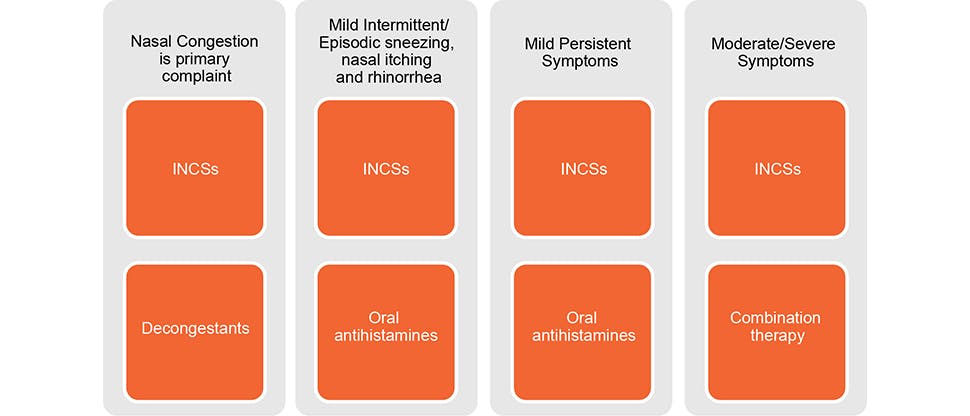
Simplified AR treatment algorithm
Although each treatment option will help to reduce a person’s AR symptoms, clinicians should tailor the treatment option. Each of the following scenarios would have different considerations2:
- Person with nasal congestion as the primary complaint
- Person with intermittent or episodic nasal AR symptoms
- Person with mild AR symptoms
- Person with moderate to severe AR symptoms
Recommendations from the AAAAI (American Academy of Allergy Asthma & Immunology)
- The American Academy of Allergy, Asthma & Immunology (AAAAI) issued practice parameters for treating rhinitis in 2008. These guidelines suggest that pharmacotherapy treatment should be individualized and depends on a variety of factors, including3:
- Type of rhinitis—seasonal allergic rhinitis (SAR), perennial allergic rhinitis (PAR), or Nonallergic rhinitis (NAR)
- Symptoms, their duration, and their severity
- Physical exam findings
- Comorbidities
- Age
- Patient preferences
Overall, the AAAAI recognizes that INCSs are an effective class for controlling symptoms of long-term treatment for AR.3
Current Canadian guidelines recommend INCSs as a first-line treatment for moderate to severe allergic rhinitis.4
Pharmacological options
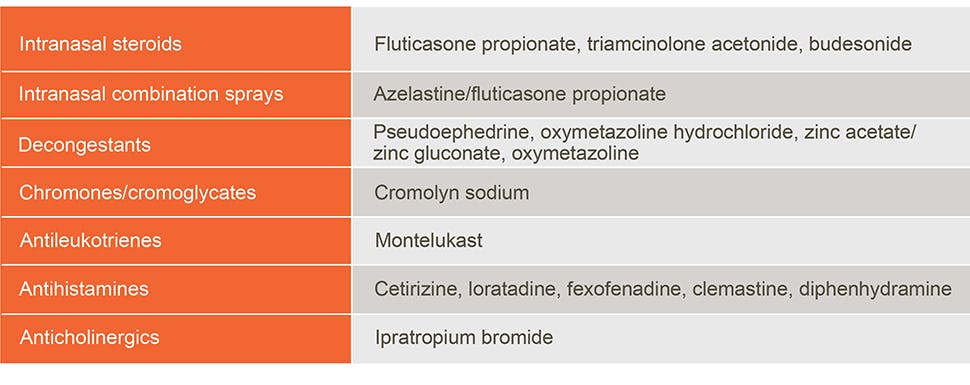
The most commonly used medications in the treatment of AR are5:
Although each treatment option will help to reduce a person’s AR symptoms, clinicians should tailor the treatment option. Each of the following scenarios would have different considerations2:
- Person with nasal congestion as the primary complaint
- Person with intermittent or episodic nasal AR symptoms
- Person with mild AR symptoms
- Person with moderate to severe AR symptoms
INCSs are considered an effective treatment for mild-persistent and moderate-severe allergic rhinitis and to help manage all nasal symptoms, ocular symptoms, polyposis, and sinusitis.7
The role of INCSs in the treatment of AR: According to the algorithms pharmacological options
According to the 2008 Rhinitis Updated Practice Parameter from the AAAAI, INCSs are an effective first-line medication class for controlling symptoms of AR.3
INCSs may provide significant symptom relief for patients with SAR, whether they’re used on a regular basis or on an as-needed basis, however continuous use may be more effective than as-needed use.3
Canadian guidelines currently mirror American and Global guidelines for treatment of AR recommending INCSs as a first-line treatment for moderate to severe allergic rhinitis.4
Read more about allergic rhinitis




Impact of Allergic Rhinitis on Patient Quality of Life
Recognize the impact allergic rhinitis has on patients’ daily lives


FLONASE® Allergy Relief
Discover how FLONASE® Allergy Relief can help reduce symptoms in your patients diagnosed with allergic rhinitis